

10 Lab Tests to Know as a Medical Student Before Clinical Rotations




Knowing the ten most commonly ordered lab tests before clinical rotations start, including their normal ranges, common abnormalities, and clinical significance, gives you immediate clinical utility on every rotation and a foundation for the clinical reasoning that attending physicians are evaluating from day one.
Stepping onto the hospital floor for the first time can be overwhelming, and one of the fastest ways to stand out as a prepared medical student is to understand common lab tests. Whether you’re evaluating a patient in the emergency department, pre-rounding on the wards, or scrubbing into surgery, knowing why a test is ordered, how to interpret results, and what it costs the patient is crucial. In this guide, we’ll break down 10 essential lab tests every M3 should master, covering their purpose, key components, turnaround time, clinical relevance, and any useful interpretation pearls. Plus, we’ll include learning strategies and pro-tips to help you apply this knowledge like a pro.
And, before we go any further, here is my first pro-tip: Avoid colloquial language! I have been burnt by this more than once on rotations. For example, don’t tell your attending you want to order “basic labs” or even “basic chest pain labs” as this means something different to everyone. Be specific, for example “I’d like to get a CMP, CBC, troponin, BNP, coagulation panel, and an EKG.” Now your attending knows that you’ve thoroughly considered what to order for this patient and more importantly, why you’re ordering it. Want to learn more about those tests I just mentioned (and a few more)? Let’s dive in!
Complete Blood Count (CBC) with Differential
Purpose: Assesses overall health, detects infections, anemia, leukemia
Key Components: White Blood Cells (WBC), Red Blood Cells (RBC), Hemoglobin (Hgb), Hematocrit (Hct), Platelets (PLT), Differential (percentage of each WBC type)
Cost to Patient: ~$10-$50
Turnaround Time: Less than 1 hour (STAT) vs. ~4-6 hours (routine)
Commonly ordered in: Every rotation!
Key Interpretations:
- An elevated WBC count (also called leukocytosis, or colloquially, a patient having a “white count”) can indicate infection, inflammation, stress, and more. It is not very specific, so use your clinical judgment when interpreting.
- A low Hgb often indicates anemia.
- Elevated platelets can indicate inflammation or something scary like malignancy, while low platelets can be seen in liver failure or bone marrow failure

Basic Metabolic Panel (BMP)
Purpose: Evaluates electrolytes, kidney function, and a cursory insight into acid-base status.
- Pro tip: When I order these for patients and they ask why, I tell them "I want to check what’s going on inside, like your ‘salts and sugars.’" Using the phrase “salts and sugars” has been highly effective for me on rotation!
Key Components: Sodium (Na), Potassium (K), Chloride (Cl), Carbon Dioxide (reported as CO2 or HCO3-), Blood Urea Nitrogen (BUN), Creatinine (Cr), Glucose, Calcium (Ca)
- Pro tip:
1) It is pronounced B-U-N not BUN as in a hotdog bun!
2) Creatinine and creatine sound similar, but are quite different!
Cost to Patient: ~$20-$60
Turnaround Time: Less than 1 hour (STAT) vs. ~4-6 hours (routine)
Commonly ordered in: Every rotation!
Key Interpretations:
- Watch out for a patient’s K (in either direction)!
- Hyperkalemia can be a sign of kidney failure and lead to the characteristic “peaked T waves” on EKG
- Hypokalemia can occur due to diuretics or gastrointestinal losses. Both are life threatening!
- Low creatinine is usually ignored, whereas a high creatinine is concerning for kidney injury (remember to compare to baseline, if you have one!)
- When evaluating glucose, consider whether the patient was fasting or not. In acute stress situations, glucose can be elevated without necessarily indicating underlying diabetes.
Fun fact: You may hear more seasoned attendings refer to this as a “Chem-7”—its old lab name, since it originally measured seven key components!
Comprehensive Metabolic Panel (CMP)
Key Components:
- BMP, plus:
- Aspartate aminotransferase (AST)
- Alanine aminotransferase (ALT)
- Alkaline Phosphatase (ALP, “alk phos”)
- Total Protein
- Albumin
- Bilirubin (“Bili”)
- Pro Tip 1: I remember that: CMP = BMP + LFTs.
- LFTs technically include all of the things mentioned above, but colloquially, it’s common to quickly refer to the AST & ALT as the “LFTs” or “liver enzymes.”
- Pro Tip 2: When I’m choosing between BMP and CMP, I ask myself:
- “Do I need to know liver function?” e.g., the patient has an underlying liver function status or I want to give them a medication that could injure the liver (e.g., antibiotics or pain relievers).
- If I really want to “dumb it down,” my rule of thumb is: If there is any pain below the diaphragm but above the belt (and especially the right upper quadrant), I get a CMP instead of BMP.
Cost to Patient: ~$20-$100
Turnaround Time: ~1-2 hours (STAT) vs. ~6-8 hours (routine)
Commonly ordered in: Every rotation, especially Internal Medicine and Emergency Medicine
Key Interpretations:
- An elevated AST/ALT is non-specific, but provides a glimpse into overall liver stress which may be caused by ischemia, hepatitis, or medications (iatrogenic).
- Bilirubin is what causes our skin to yellow (jaundice). Usually an elevated conjugated bilirubin is a worse indicator than elevated unconjugated bilirubin because I am concerned about the liver’s ability to excrete bile.
Fun Fact: You may hear more seasoned attendings refer to this as a “Chem-10,” because again, that was its former lab name when it measured 10 key components!
Urinalysis (UA) with Microscopy
Purpose: Evaluates kidney function, detects infections, looks for blood or protein in the urine
Key Components:
- Physical Examination: Color, Clarity, Volume, Odor, Specific Gravity
- Chemical Examination: pH, Cells, Proteins, Glucose, Bilirubin, Nitrites, Leukocyte Esterase
- Microscopic Examination: Casts, Crystals, Microorganisms
Cost to Patient: ~$10-$30
Turnaround Time: ~1-2 hours (STAT) vs. ~4-6 hours (routine)
Learning Tip:
There is a spectrum of urinalysis:
- Urine dipstick test: results appear rapidly, less accurate
- Urinalysis: standard test
- Urinalysis with microscopy: more detailed examination
- Urine culture: takes 1-2 days, not always necessary
Commonly ordered in: Internal Medicine, Pediatrics, Emergency Medicine
Key Interpretations:
- Having a positive leukocyte esterase and/or nitrites should tip you off that there might be a urinary tract infection (UTI)!
- Leukocyte esterase is produced by WBCs in response to an infection indicating presence of WBCs in the urine (pyuria).
- Nitrites are produced by certain bacteria, namely gram-negatives, that have the enzyme nitrate reductase.
- UAs will also measure the amount of squamous epithelial cells, which are the skin cells around the area of collection. A high amount (usually >5) indicates likely contamination or a “not-clean sample.” Interpret your results with caution!
- Presence of blood in the urine (hematuria) should concern you for UTIs, kidney stones, or trauma.
Troponin
Purpose: Detects myocardial injury, essential in chest pain workup
Key Components: Troponin I and Troponin T
Learning Tip:
- Troponin I and Troponin T are cardiac-specific proteins used to detect myocardial injury.
- These days, the high-sensitivity cardiac troponin (hs-cTn) is now the most commonly used troponin assay.
Cost to Patient: ~$30-$100
Turnaround Time: Less than 1 hour (STAT) vs. ~2-4 hours (routine)
Commonly ordered in: Internal Medicine, Emergency Medicine
Key Interpretations:
- Please pay attention to what troponin test your hospital’s lab uses, as this greatly affects the reference range!
- Elevated troponin is concerning for acute myocardial ischemia but can be seen in many conditions that may affect the heart’s ability to function, such as a pulmonary embolism, congestive heart failure, chronic kidney disease, and other conditions affecting cardiac function.
- Clinical gestalt (a.k.a. your overall impression or intuitive judgment) is paramount in troponin testing. Consider the following scenarios:
- Case: A young 24-year-old male presents with chest pain after a wrestling tournament. Troponin is 0.
- Interpretation: In this scenario, the troponin was ordered because of the chest pain (we can’t miss a heart attack) but, since it was zero and they are very low risk (See HEART Pathway for Early Discharge in Acute Chest Pain), MI is very unlikely.
- Case: A 58-year-old male with crushing substernal chest pain, diaphoresis, nausea, and vomiting, with a history of hypertension, hyperlipidemia, and diabetes.
- Interpretation: This patient absolutely needs a troponin (and EKG) as they are high-risk for acute coronary syndrome!
- Case: A 70 year old male with a history of a prior myocardial infarction and comorbid heart failure and chronic kidney disease.
- Interpretation: This patient’s troponin is likely chronically elevated and you must consider the patient’s presenting symptoms, exam, and baseline to determine how to interpret a troponin in this patient.
- Case: A young 24-year-old male presents with chest pain after a wrestling tournament. Troponin is 0.
- Lastly, we often order repeat troponins (also called serial troponins) to assess for a trend (often called “delta”). Troponin levels should be measured at presentation and 3 to 6 hours after symptom onset in all patients who present with symptoms consistent with ACS to identify a rising and or falling pattern. (Level of Evidence: A)
Coagulation Panel
Purpose: Assesses clotting function and monitors anticoagulation therapy (e.g., warfarin, heparin).
Key Components: Prothrombin Time (PT), Activated Partial Thromboplastin Time (aPTT), International Normalized Ratio (INR), Fibrinogen
Pro-Tip: Depending on the hospital or clinical setting, a coagulation panel may also include: Platelet Count, D-Dimer, Thrombin Time, or specific coagulation factor assays
Learning Tip: PT measures the extrinsic side of the coagulation cascade (namely Factors III and VII) whereas aPTT measures the intrinsic side of the cascade (namely Factors IX through XII).
Cost to Patient: ~$20-$60
Turnaround Time: Less than 1 hour (STAT) vs. ~4-6 hours (routine)
Commonly ordered in: Surgery, Internal Medicine, Emergency Medicine
Key Interpretations:
- Elevated PT/INR can be a desired effect of the anticoagulant warfarin (which, among other things, impairs Factor VII and prolongs clotting time)
- Elevated aPTT can be a desired effect of heparin or signify a lack of intrinsic pathway coagulation factors.
D-Dimer
Purpose: Helps rule out venous thromboembolism (VTE) in low-risk patients
Key Components: D-dimer (it’s just one test measuring one thing!)
Learning Tip: Recall what the D-dimer even is! It’s a protein fragment produced when a blood clot breaks down. Scary to think about, but our bodies are forming and breaking down clots all the time, so some level of d-dimer is to be expected. It’s usually undetectable on lab testing in normal circumstances.
Cost to Patient: ~$100-$300
Turnaround Time: ~1-2 hours (STAT) vs. ~4-6 hours (routine)
Commonly ordered in: Internal Medicine, Emergency Medicine
Key Interpretations:
- Elevated D-dimer is concerning for significant blood clotting such as a deep vein thrombosis, pulmonary embolism, or disseminated intravascular congestion
- A negative D-dimer helps reassure you or “rule-out” a blood clot in a low-risk patient
Pro Tip: Before asking your resident or attending for a D-dimer, consider its purpose and next steps:
- When that D-dimer comes back elevated, there’s more testing to be done such as a Doppler ultrasound of the legs or a CT scan looking for a pulmonary embolism.
- Before ordering the D-dimer, consider a clinical calculator, such as the Wells' Criteria for Pulmonary Embolism, which can help determine if ordering a D-dimer is supported by objective data.
- You may also consider the PERC Rule for Pulmonary Embolism for patients who are low risk— if they meet one ore more PERC criteria, a D-dimer may be warranted.
Learning Tip: Common false positives on D-dimer testing include: surgery, trauma, pregnancy, obesity, advanced age, infections, and heart disease.
Lactate
Purpose: A marker of tissue hypoxia, sepsis, or shock.
Key Components: Lactate (it’s just one test measuring one thing!)
Learning Tip: Elevated lactate can be the result of increased lactic acid production, decreased lactic acid clearance, or a mixture of both.
Cost to Patient: ~$50-$100
Turnaround Time: Less than 1 hour (STAT) vs. ~2-4 hours (routine)
Commonly ordered in: Surgery, Internal Medicine, ICU, Emergency Medicine
Key Interpretations:
- Lactates are fairly non-specific—it tells me that there’s some degree of acute stress on the body, leading some cells to switch to anaerobic metabolism.
- Elevated lactate levels are concerning for: tissue hypoperfusion, sepsis, shock, lactic acidosis, diabetic ketoacidosis, toxins and pharmacological agents, malignancies, liver failure, and much more!
Arterial Blood Gas (ABG)
Purpose: Evaluates oxygenation, ventilation, and acid-base balance.
Key Components: pH, pCO2, pO2, Bicarbonate (HCO3-), Base Excess
Cost to Patient: ~$50-$200
Turnaround Time: ~15-30 minutes if done STAT at the bedside
Commonly ordered in: Internal Medicine, ICU, Emergency Medicine
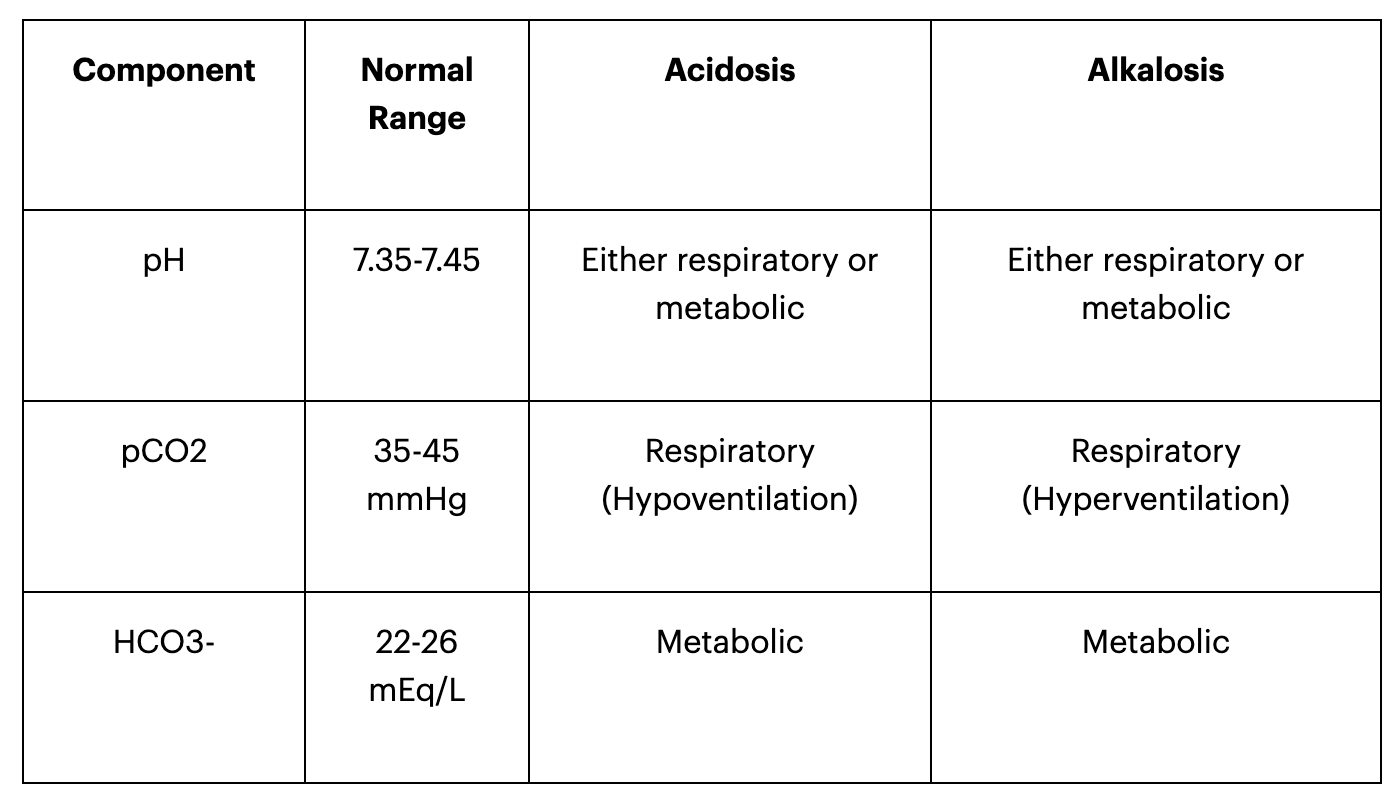
Key Interpretations:
- An ABG is one of the best ways to acutely look at a patient’s acid-base status which is critical in many conditions, such as acute respiratory distress syndrome, heart failure, diabetic ketoacidosis, severe sepsis or septic shock.
- Interpreting an ABG is a 10-hour long conversation best done by an ICU physician but, here’s a quick refresher on the physiology behind blood gasses:
Blood Cultures
Purpose: Detects bloodstream infections and guides antibiotic therapy
Key Components:
- Usually collected as a set of two from separate sites
- Bottles vary and can be aerobic, anaerobic, pediatric, or specialized each with their own growth media and anticoagulants
Pro Tip: Draw blood cultures before starting antibiotics, from two separate sites
Cost to Patient: ~$50-$250
Turnaround Time:
- Preliminary: ~24 hours
- Final result: 48-72 hours
- If positive, pathogen ID and sensitivities take another 24-48 hours
Commonly ordered in: Internal Medicine, ICU, Emergency Medicine
Key Interpretations:
- True Positive:
- The patient is acutely ill, meets sepsis criteria, and blood cultures return positive (often quickly!); indicates that some kind of bacteria is in the bloodstream (bacteremia).
- Start empiric broad-spectrum antibiotics if you haven’t already, and wait for sensitivities to narrow down antibiotics.
- If you see these bugs in a blood culture, be very concerned as it is likely a true bloodstream infection:
- Staphylococcus aureus (the most common cause of true bacteremia), Streptococcus pneumoniae, Escherichia coli (the most common gram-negative bacteria isolated from blood cultures), Candida albicans, Listeria monocytogenes, Neisseria meningitidis, Neisseria gonorrhoeae
- False Positive:
- The most common pathogen found in false positive blood cultures is coagulase-negative staphylococci (CNS), particularly Staphylococcus epidermidis, which is usually found on the skin and may have been introduced during collection.
- Other common contaminants that can lead to false positive blood cultures include: Corynebacterium spp., Bacillus spp., Micrococcus spp., Propionibacterium acnes, and Viridans group streptococci
- True Negative:
- This is reassuring! Although, if suspicion remains high, such as another febrile episode in a hospitalized acutely ill patient, consider repeat blood cultures.
Additional Important Lab Tests
While these may not have made the top 10, they are commonly ordered and useful to know:
- Magnesium (Mg) & Phosphorus (Phos) – Important for electrolyte balance, especially in ICU patients
- C-Reactive Protein (CRP) & Erythrocyte Sedimentation Rate (ESR) – Non-specific inflammatory markers
- Procalcitonin – Helps differentiate bacterial vs. viral infections
- B-Type Natriuretic Peptide (BNP) – Marker for heart failure
- Ammonia – Assesses hepatic encephalopathy
- Lipase & Amylase – Evaluates for pancreatitis
- Hemoglobin A1c (HbA1c) – Monitors long-term blood sugar control in diabetics
- Thyroid Function Tests (TSH, Free T4, Free T3) – Evaluates thyroid disorders
- Ferritin, Iron, Total Iron Binding Capacity (TIBC) – Workup for anemia
- Vitamin B12 & Folate – Identifies deficiencies causing macrocytic anemia
- Urine Drug Screen (UDS) – Detects common substances in cases of suspected overdose or toxicity
- Lipid Panel – Assesses cholesterol levels
- CSF Analysis (Cell count, Protein, Glucose, Gram stain, Culture, PCRs) – Workup for meningitis/encephalitis
- Hepatitis Panel (Hep A, B, C serologies) – Evaluates for liver infections
- HIV & Syphilis Testing (HIV Ab/Ag, RPR/VDRL, FTA-ABS) – Workup for infection or new diagnosis
