

How to Build Clinical Reasoning Skills in Medical School




Clinical reasoning is the most important skill you develop in medical school, and it is built through deliberate practice, not passive exposure. Illness script development, thinking out loud during presentations, and reading on your own patients are the highest-leverage habits for building it systematically.
For many medical students, the transition from book-based learning to Case-Based Learning (CBL) can feel daunting. Which reminds me, when was the last time you opened up a book in medical school? Mine was the first week of medical school! The first two years of medical school often emphasize rote memorization, fact retention, and textbook-heavy study habits. Thankfully, in 2025 we have memory aids such as Sketchy to make acquiring this foundational knowledge much easier. However, as students progress, they must begin thinking like doctors—in other words, applying “book” knowledge to clinical scenarios, developing differential diagnoses, and making patient-centered decisions (i.e. clinical reasoning skills). It all comes down to the application of what you spent so many hours learning.
In essence, CBL is designed to bridge the gap between theoretical learning and real-world application. Instead of passively absorbing information, students engage with cases that simulate actual patient encounters, requiring them to analyze symptoms, prioritize next steps, and think critically. This blog will explore how to successfully shift from book-based learning to case-based learning, providing practical strategies to develop a clinical mindset and excel in case-based discussions.
What is CBL and How is it Typically Structured?
Zhao et al.1 define case-based learning as an educational method grounded in the analysis of medical records, which is designed to recreate clinical scenarios and prompt students to identify and develop new areas of learning. Students are presented with patient cases, which prompts them to engage in active problem-solving rather than passive studying. Unlike traditional lecture-based learning, where information is delivered in a linear format, CBL requires students to build those clinical reasoning skills, to critically assess patient presentations, formulate differential diagnoses, and determine appropriate diagnostic and management steps. Interestingly enough, the first evidence of CBL was introduced back in 1912 by Dr. James Lorrain Smith, long before what we know as modern medical education was established.2 In 1920, the Harvard Business School adopted the case-based learning method and continues to use it to this day.3 Little did Dr. Smith know that CBL would become a mainstay of medical education.
If you’ve read any of my other blogs (thank you!), you know I’m a sucker for data.
I won’t bore you with too much here—and feel free to follow the citations to read more in depth—but multiple studies have found that CBL enhances medical student and resident clinical practice, problem-solving, and analytical skills.4 Overwhelmingly, studies have shown that students think very highly of CBL, enjoy the degree of creativity and challenge, and prefer electronic CBL methods5 overall.
Another thing to consider is the rapid expansion of accessible information due to the Internet. Since e-learning is a mainstay of undergraduate medical education, especially during and after the COVID-19 pandemic, electronic CBL helps medical students effectively obtain information (even with limited timeframes) and allows them to actively think and ask questions, while also guiding them in the acquisition of new information.6
CBL sessions are typically conducted in small groups or by using virtual platforms, with students working together or independently to analyze cases under the guidance of a facilitator. While structures can vary, most CBL sessions follow a common format:
- Pre-Session Preparation: Students are often encouraged to review key concepts related to the upcoming case, allowing them to contribute meaningfully to discussions.
- Progressive Disclosure: The case unfolds gradually, simulating how doctors gather information over time. Students receive or inquire about the initial patient presentation, discuss possible differentials, and then obtain additional history, physical exam findings, and test results in stages.
- Interactive Discussion: Facilitators guide students through the case, prompting them to justify their reasoning and explore alternative possibilities.
- Post-Session Reflection: After the session, students review knowledge gaps, research unclear topics, and consolidate learning to reinforce clinical reasoning.
CBL is particularly valuable because it mirrors real-world medical practice, where physicians must assess evolving patient data and make informed decisions.
Why It’s Important to Start Early
Many students approach CBL passively, expecting to absorb knowledge just by participating in discussions. However, actively engaging in case-based learning from the beginning of medical school can yield tremendous benefits:
- Bridges the Gap Between Preclinical and Clinical Years: Instead of viewing basic sciences as isolated facts, CBL helps integrate subjects like physiology, pathology, and pharmacology into clinical reasoning. This makes the transition to clinical rotations smoother.
- Enhances Critical Thinking and Diagnostic Skills: CBL forces students to think beyond memorized facts, teaching them to develop differential diagnoses and prioritize management decisions. This is especially important as patients rarely present as the textbook describes it—darn, patients!
- Develops Team-Based Learning and Communication Skills: Working in small groups encourages collaborative learning, a crucial skill for future clinical practice.
- Prepares Students for Step Exams and Clinical Rotations: Since exams like the USMLE increasingly emphasize clinical vignettes, engaging in case-based learning early helps students develop the test-taking strategies needed for success.
Starting early with an active approach to CBL ensures that students like yourself internalize clinical reasoning skills before stepping into patient care settings.
How to Maximize your Time during CBL
To maximize the benefits of CBL, follow some of these tips & tricks:
- Review core topics related to the upcoming case. If the case involves a patient with chest pain, ensure you understand cardiac physiology, ischemic heart disease, and common differentials.
- Familiarize yourself with standard diagnostic workups for relevant conditions. This can be very difficult in your preclerkship years, but will get easier the more time you spend in the hospital.
- Approach preparation as if you were responsible for diagnosing and treating the patient in real life.
- Engage actively by asking questions and contributing ideas.
- Think out loud—verbalizing reasoning helps refine clinical decision-making.
- Challenge yourself by considering alternative diagnoses and asking, “What’s the next step?”
The learning doesn’t stop once the case has been solved. Focus on identifying knowledge gaps and reviewing unclear concepts you encountered. Rely on the trust flowchart or concept map to summarize key takeaways. And, like everything in medicine, repetition is key. Practice similar cases and engage in practice questions to reinforce your learning.
Effective Strategies for Succeeding in CBL
Adjusting from book-based learning to case-based learning is no small feat - but building strong clinical reasoning early is what sets great med students apart! Here are a few tips I have for making the transition:
- Adopt a Clinical Mindset Early: Approach cases as if you were responsible for the patient’s care. This is the biggest tip I give almost all medical students—the more you buy-in, the bigger your learning return is.
- Use Clinical Frameworks: Apply systematic methods like the VINDICATE mnemonic for differentials.
- Be Comfortable with Uncertainty: Medicine isn’t about finding one correct answer—developing a thoughtful approach is more important.
- Tie Cases to Real-World Experiences: If you’ve encountered a similar case on rotations, draw connections to deepen your understanding.
Challenges in Transitioning to CBL / Common Mistakes and How to Avoid Them
The transition to CBL presents unique challenges for medical students. One of the most common mistakes is over-relying on memorization rather than applying foundational knowledge to real clinical scenarios. While memorization has its place, and is made much easier because of Sketchy, true clinical reasoning requires integrating basic science concepts with patient presentations. Additionally, many students avoid uncertainty, fearing that not knowing an answer reflects a lack of understanding. However, uncertainty is an inherent part of medicine, and learning to navigate it is essential for developing problem-solving skills. Lastly, failing to consolidate learning after CBL sessions can hinder long-term retention, as students may move on without fully reinforcing key takeaways.
To overcome these challenges, you should prioritize clinical reasoning over rote memorization by consistently asking yourself why a disease presents a certain way and how different pathophysiologic processes interact. Approaching CBL sessions as active learning opportunities—rather than passive exercises—helps maximize engagement and reinforces a structured thought process. Rather than shying away from uncertainty, students should embrace it as a critical part of medical learning, using it as a prompt to seek deeper understanding. Finally, reviewing each case after the session and connecting it to related topics solidifies knowledge, enhances retention, and builds a more comprehensive understanding of clinical medicine. By shifting their mindset and study approach, students can successfully transition to CBL and develop the problem-solving skills necessary for both patient care and exam success.
Step Exam Integration: How CBL Prepares You for USMLE Success
The benefits of CBL don’t just help with your in-house exams or on rotations. It is an excellent way to prepare for the USMLE and/or COMLEX exams, as both emphasize clinical reasoning through patient vignettes. The transition from preclinical learning to board exam preparation can feel overwhelming, but engaging with CBL early fosters the skills necessary for success. Much like the Step 1 and Step 2 CK exams, which require analyzing patient cases using clinical reasoning to determine diagnoses and management plans, CBL encourages students to systematically break down patient presentations by integrating knowledge from the basic and clinical sciences. This habit of structured thinking enhances test-taking performance by making complex cases more approachable and manageable.
One of the most valuable skills developed through CBL is the ability to identify key diagnostic clues within a clinical scenario—just as board exam questions require you to recognize critical signs, symptoms, and lab findings to arrive at the correct diagnosis. Additionally, CBL refines decision-making skills, which are essential not only for answering test questions efficiently but also for real-world clinical practice. Students who actively engage in case discussions develop a deeper understanding of disease mechanisms, treatment rationales, and the reasoning behind clinical guidelines, all of which translate directly to board exam success.
By applying CBL principles to practice questions, students reinforce their ability to approach clinical vignettes methodically and strengthen their diagnostic and management skills. This integrated approach ensures that when their test day arrives, they are not only recalling isolated facts but thinking like a physician—an essential mindset for excelling on the USMLE and beyond.
Conclusion
The shift from book-based learning to CBL can feel overwhelming, but embracing it early fosters essential clinical reasoning skills. By integrating basic science knowledge with real-world cases, students strengthen their diagnostic abilities and prepare effectively for both patient care and board exams. CBL isn't just about learning medicine—it's about thinking like a doctor.
Example Case Scenario Walkthrough: Chest Pain in a Middle-Aged Man (Integrating Basic Science Concepts)
Case Presentation:
A 55-year-old male presents to the emergency department with crushing substernal chest pain radiating to his left arm for the past 30 minutes. He describes it as "a heavy weight" on his chest. He has a history of hypertension, hyperlipidemia, and smoking. His vitals show BP 145/90 mmHg, HR 95 bpm, RR 18, SpO₂ 98% on room air.
Step 1: Formulating a Differential Diagnosis:
Before jumping into the workup, we apply foundational pathophysiology and anatomy concepts to generate a broad differential diagnosis.
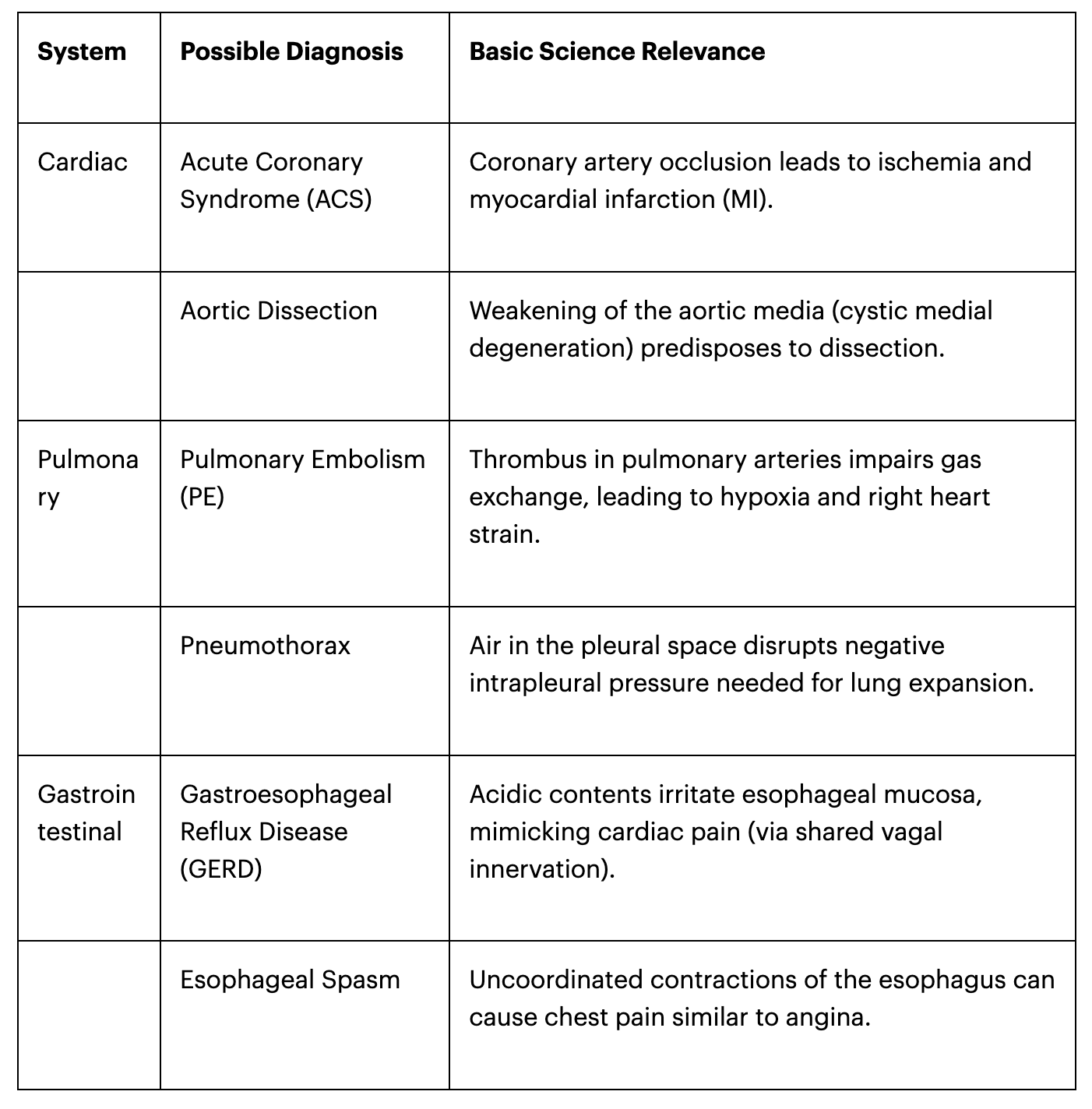
Key takeaway: Understanding the embryology and autonomic innervation of the thorax helps differentiate cardiac vs. non-cardiac causes of pain. The heart and esophagus share vagal afferents, explaining why esophageal pain can mimic angina.
Step 2: Understanding the Pathophysiology of Acute Coronary Syndrome (ACS)
Since ACS is the most likely diagnosis, we apply basic science principles to understand how an MI develops.
- Vascular Pathology & Histology
- Atherosclerosis: Chronic inflammation leads to lipid-laden macrophages (foam cells) forming fatty streaks, which progress to plaques.
- Plaque Rupture & Thrombosis: A vulnerable plaque (thin fibrous cap, lipid-rich core) ruptures, exposing subendothelial collagen and tissue factor, triggering platelet adhesion and clot formation.
- Myocardial Ischemia & Metabolism
- Oxygen supply-demand mismatch: If coronary occlusion persists, myocardial oxygen supply cannot meet demand, leading to anaerobic metabolism and lactate accumulation (basis of ischemic chest pain).
- Cellular Injury Progression:
- 0–30 min: ATP depletion → Reversible injury.
- 30 min–4 hrs: Irreversible damage, membrane rupture.
- 4–12 hrs: Coagulative necrosis, release of troponins (biomarker for MI).
- 12–24 hrs: Neutrophilic infiltration.
- 3–5 days: Macrophage infiltration (risk of ventricular free wall rupture).
- Autonomic Influence on Symptoms
- Sympathetic activation (due to pain/stress) leads to diaphoresis, tachycardia, and hypertension—hallmarks of an MI.
- Referred pain to the left arm occurs via the T1-T5 dermatomes, which transmit visceral afferents from the heart.
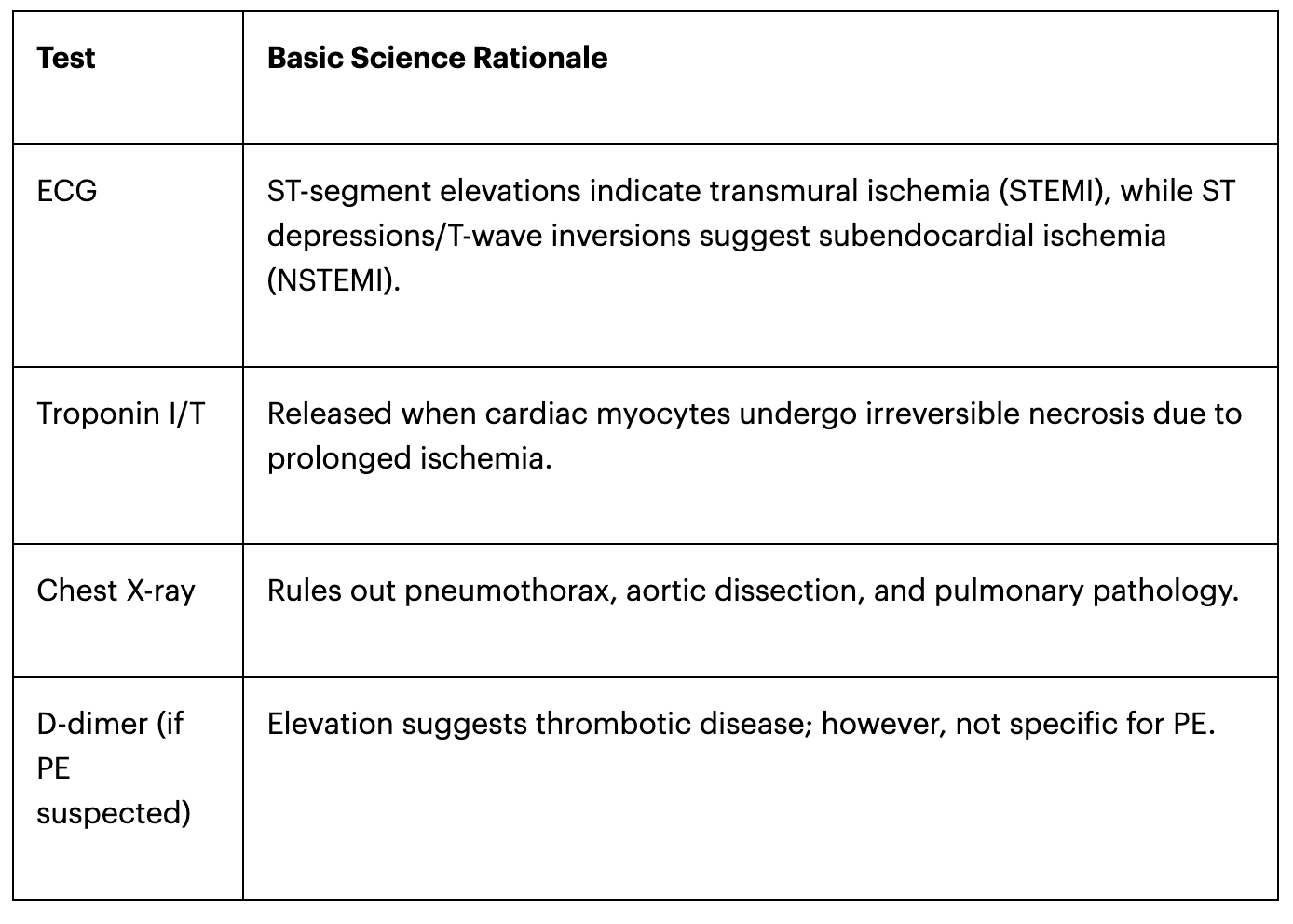
Step 3: Determining the Initial Workup
Applying clinical pathology principles, we order key tests:
Step 4: Management Plan (Tying in Pharmacology & Physiology)
If STEMI is confirmed:
1. Reperfusion Therapy
Percutaneous Coronary Intervention (PCI) to reopen the blocked artery.
Fibrinolytics (tPA) if PCI unavailable, breaking down fibrin in the thrombus.
2. Pharmacologic Management:
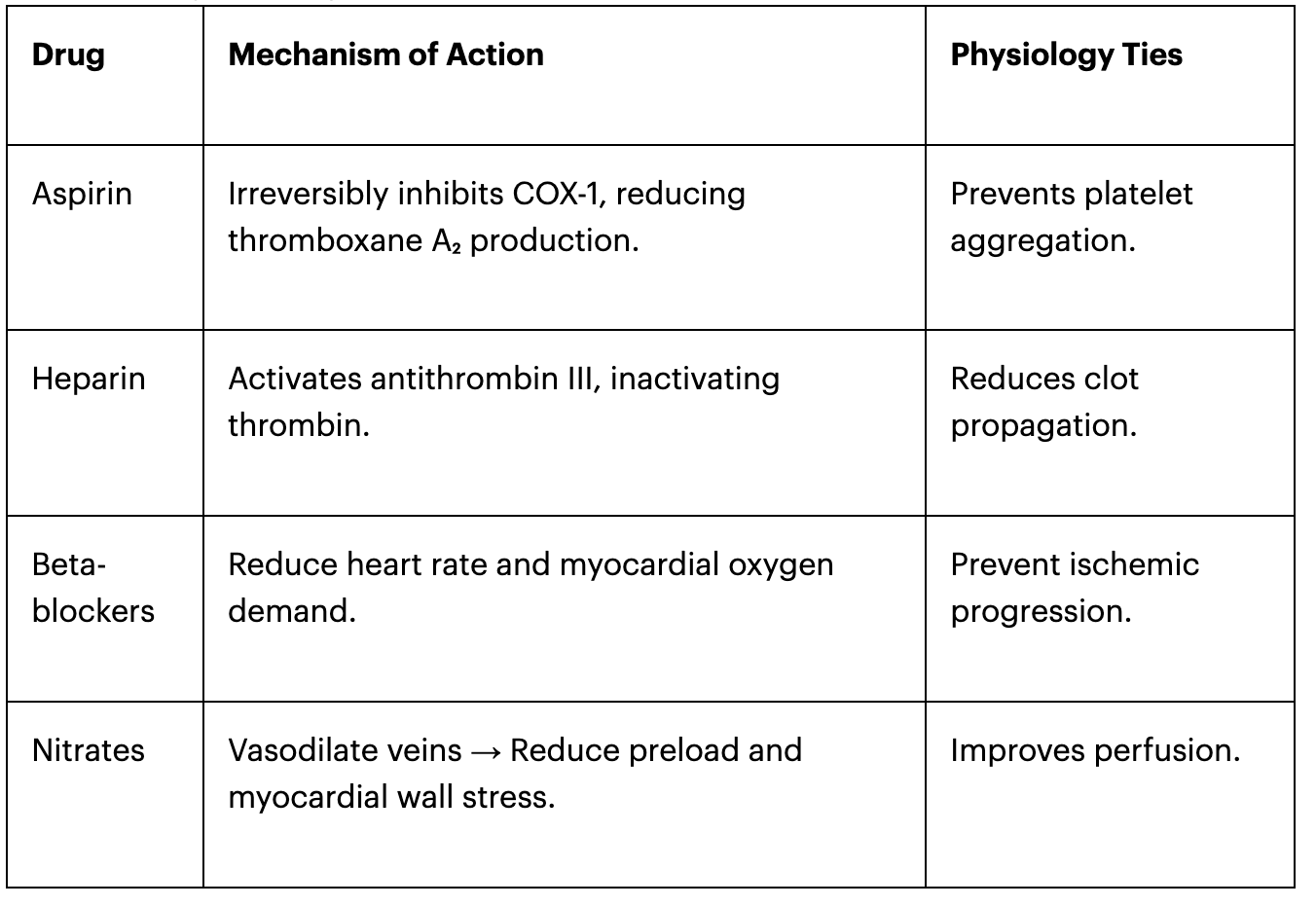
3. Post-MI Complications (Pathology Considerations)
- Papillary muscle rupture (3-5 days) → Leads to mitral regurgitation.
- Ventricular free wall rupture (5-7 days) → Causes cardiac tamponade.
- Pericarditis (1-2 weeks, Dressler’s syndrome) → Autoimmune reaction causing inflammation.
Bridging to Step Exams and Clinical Rotations
How This Case Helps on Step Exams:
- Step 1: Understanding the pathophysiology of myocardial ischemia, ATP depletion, and histologic changes.
- Step 2: Applying clinical reasoning to distinguish MI from other causes of chest pain.
- Step 3: Choosing the appropriate management plan, including emergency interventions and pharmacologic therapy.
Practicing cases like this helps students develop a systematic approach to clinical problem-solving, making CBL an essential tool for both real-world medicine and exam success.
Common questions

1 Zhao, W., He, L., Deng, W. et al. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ 20, 381 (2020). https://doi.org/10.1186/s12909-020-02306-y
2 Sturdy S. Scientific Method for Medical Practitioners: The case method of teaching pathology in early twentieth-century Edinburgh. Bull Hist Med 2007; 81(4)760–792
3 Thistlethwaite, J. E., Davies, D., Ekeocha, S., Kidd, J. M., MacDougall, C., Matthews, P., … Clay, D. (2012). The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Medical Teacher, 34(6), e421–e444. https://doi.org/10.3109/0142159X.2012.680939
4 Williams B. Case based learning—a review of the literature: is there scope for this educational paradigm in prehospital education? Emerg Med J. 2005;22(8):577–81.
Nair SP, Shah T, Seth S, Pandit N, Shah GV. Case based learning: a method for better understanding of biochemistry in medical students. J Clin Diagn Res Jcdr. 2013;7(8):1576–8.
5 Thistlethwaite, J. E., Davies, D., Ekeocha, S., Kidd, J. M., MacDougall, C., Matthews, P., … Clay, D. (2012). The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Medical Teacher, 34(6), e421–e444. https://doi.org/10.3109/0142159X.2012.680939
6 Schittek M, Mattheos N, Lyon H, Attström R. Computer assisted learning. A review. Eur J Dent Educ. 2001;5(3):93–100.
Hendricson WD, Panagakos F, Eisenberg E, McDonald J, Guest G, Jones P, Johnson L, Cintron L. Electronic curriculum implementation at north American dental schools. J Dent Educ. 2004;68(10):1041–57.
